Good medical records are more than just documentation -they are the backbone of quality care, legal protection, patient rights, and regulatory compliance. A comprehensive record ensures that every decision, treatment, and outcome is traceable, protecting both patients and providers. In today’s healthcare landscape, effective medical documentation plays a critical role in preventing medical negligence claims.
As the healthcare sector becomes more complex, the stakes are higher than ever. With the widespread adoption of digital health records, stricter regulations, and increasing audit readiness requirements, the integrity of medical documentation has become a critical factor in both healthcare delivery and medico-legal proceedings. Accurate, accessible, and well-maintained documentation not only supports continuity of care but also serves as powerful evidence in legal disputes and compliance audits.
Partner with us for top-notch medical review services!
Call (800) 670-2809
Role of Medical Records in Medico-legal Cases
From a legal viewpoint, accurate record-keeping works in the provider’s favor if they need to respond to or defend against a complaint or claim. In negligence cases, contemporary clinical notes of all decisions made about a patient’s care -and the reasoning behind those decisions – are vital.
In medico-legal proceedings, these records serve as invaluable documents that provide a comprehensive and accurate account of a patient’s medical history, diagnoses, treatments, and outcomes. They establish a clear timeline of events, aid in determining liability, and serve as credible evidence in court.
Medical records not only document the patient’s condition but also capture the healthcare provider’s observations, assessments, and decisions. This allows legal professionals and expert witnesses to assess the standard of care provided, identify deviations, and determine whether negligence or malpractice occurred.
Though highly confidential, records may be released for legitimate purposes with proper authorization from the patient or their representative. Providers must ensure that documentation thoroughly captures patient progress, decisions made, and supporting evidence. This level of detail facilitates communication with future treating physicians and strengthens the record’s value in both medical and legal contexts.
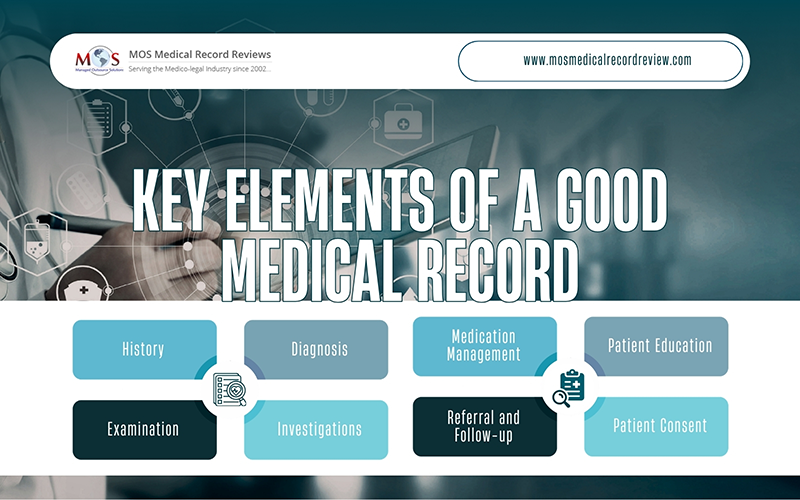
What Constitutes a Good Medical Record in Healthcare?
A good medical record should be comprehensive and accessible, legible and properly dated. Good note taking is very important.
The following aspects should be clearly recorded.
- History: This refers to the condition of the patient and relevant past history including concurrent illnesses, medications prescribed, and allergies if any.
- Clinical Examination Findings: Must contain all positive and applicable negative findings, all pertinent observations and measurements including temperature, blood pressure, and pulse.
- Diagnosis: The diagnosis made must be accurately recorded, showing the reason for making such a diagnosis. Any differentials or uncertainties must be clearly recorded.
- Investigations: These should include all imaging tests such as X-rays or scans, and all lab results.
- Medication Management: These records should provide information regarding the drugs prescribed and administered with dosage. Information about other treatments such as physiotherapy must also be given.
- Referral and Follow-up: Any follow-up tests recommended, future appointments made, and referrals must be mentioned clearly.
- Patient Education: Here all details of discussions with the patient regarding risks and benefits of the treatment, treatment plan, prognosis, and potential complications should be recorded.
- Patient Consent: The consent given by the patient must be recorded, making sure that it takes into account all the above-mentioned aspects.
When considering the medical record as a legal document, complete and accurate documentation is the best alibi for the provider and can stop a medico-legal claim from proceeding any further.
Well-prepared patient files will contain answers to the fundamental questions such as who (details of the patient who was provided the treatment or service, the providers who administered the treatments), when (the date and time when the patient was seen or when a test or other procedure was undertaken, or a treatment given), what (what was done, said, observed, instructed, or checked) and why (justification regarding why the decisions were taken with regard to patient care).
An important thing for providers to note is that any improper alteration of the medical records with a view to mislead the parties and the court in legal proceedings could lead to serious admonishment by a court. It could also prove to be the ground for regulatory criticism on occasions where there is a duty to maintain accurate medical records.
Consistent and clear medical documentation is crucial for effective defense in legal cases, providing a comprehensive understanding of patient care. Such records benefit the medical team, the patient, courts, and healthcare providers in explaining and defending actions during legal proceedings.
Documentation Best Practices for Legal and Clinical Protection
Given the importance of medical records as legal documents, providers must follow clear and consistent documentation practices. Strong documentation not only supports patient care but also protects against legal challenges.
Key principles include:
- Clarity over ambiguity: Avoid vague notes or shorthand that could be misinterpreted. Every entry should be precise and understandable to other practitioners and legal reviewers.
- Chronological consistency: Dates and sequences must be accurate. A clear timeline strengthens evidentiary narratives and prevents confusion in court.
- Objectivity over subjectivity: Medical documentation should remain factual and free of personal opinions. Objective documentation carries greater weight in legal proceedings.
- Comprehensive coverage: Ensure all consultations, lab results, procedures, and follow-up instructions are documented in the formal clinical record.
- Proper dating and signatures: Entries must be time-stamped, signed, and verified to establish authenticity.
- Standardized abbreviations: Use only widely accepted abbreviations so that records are easily understood by other providers and legal professionals.
By adhering to these best practices, healthcare providers strengthen the integrity of medical records, ensuring they serve as reliable evidence in medico-legal cases and compliance audits.
Common Documentation Errors That Compromise Legal Defensibility
Even well-intentioned documentation can lose its legal strength if certain errors creep in. These mistakes weaken credibility, create confusion, and may even render records inadmissible in court. Common pitfalls include:
- Missing dates or incomplete entries: Without precise timestamps, the sequence of care becomes unclear.
- Inconsistent terminology: Using different terms for the same condition or treatment undermines clarity.
- Illegible handwriting or poor coding: Records that cannot be read or properly interpreted lose evidentiary value.
- Alterations without audit trails: Changes made without clear version history or justification raise suspicion of tampering.
- Unsigned or undated entries: Lack of authentication makes it difficult to prove who documented the care and when.
- Subjective or biased language: Personal opinions or vague descriptions weaken the factual basis of records.
- Duplicate or conflicting documentation: Multiple versions of the same event create confusion and reduce reliability.
- Failure to record follow-up instructions: Missing details about next steps can be construed as negligence.
Avoiding these errors ensures medical records remain credible, defensible, and useful in both patient care and legal proceedings.
How AI is Enhancing Medical Records Quality and Legal Preparedness
The rise of AI in healthcare documentation is transforming how medical records are created, maintained, and reviewed. By combining automation with expert oversight, AI strengthens both clinical accuracy and legal defensibility.
- AI-driven extraction: Automatically identifies and pulls key data such as dates, diagnoses, treatments, and outcomes from raw records, reducing manual effort.
- Smart integrity checks: Flags gaps, inconsistencies, or missing signatures that could compromise the legal strength of records.
- Automated audit trails: Tracks edits, versions, and sources during medico-legal review, ensuring transparency and defensible documentation.
- AI-assisted summarization: Generates summaries, timelines, and chronologies quickly, helping legal teams and providers avoid fatigue while maintaining precision.
By integrating these capabilities, healthcare providers and legal professionals gain records that are not only comprehensive but also optimized for compliance, litigation, and patient safety.
As mentioned earlier, medical records are important evidence in medical negligence and injury claims and must therefore be carefully written and maintained. During a medical record review, the medical chart should provide clear, accurate, chronological, consistent, and complete details about the patient care provided. A medical review company can extend that much-needed helping hand to attorneys, saving them from the trouble of deciphering complex medical records. Professional medical review professionals can efficiently handle all the above and other issues related to patient records because reviewing medical records is their core task, to carry out which they have the necessary prowess, time, and dedication.
With AI-enabled review processes, these companies further enhance accuracy and efficiency – automatically detecting gaps, inconsistencies, and sequencing errors while generating streamlined timelines. This hybrid of expert analysis and AI support ensures records are not only legally defensible but also optimized for faster case preparation.
Revolutionize your legal strategy with our AI-driven medical review services, delivering accuracy, speed, and defensible documentation.
Request a consultation today at (800) 670-2809!